Cervical cancer is caused by persistent infection with high-risk human papillomavirus (hrHPV). In 2008, Harald zur Hausen, a German virologist, won the Nobel Prize in Physiology and Medicine for establishing the link between high-risk genital HPV infection and cervical cancer.
HPV transmission is mainly by sexual contact and hence many women become infected within a few years after sexual debut. HPV is the most common sexually transmitted infection worldwide. Up to 80% of women will at some point in their life have an HPV infection.
Accordingly, the main risk factors for HPV infection are defined by sexual (risk) behavior, including life time number of sexual partners and the acquisition of new male partners. HPV prevalence is also high among persons with an immune disorder, such as HIV.
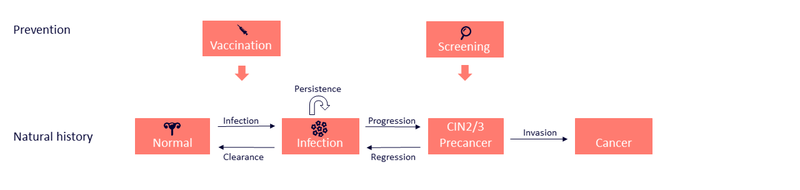
The majority of HPV infections clear spontaneously and only 5 to 10 percent becomes persistent. These persistent infections may progress to cancer which takes at least 12 years.
Squamous cell carcinomas develop through premalignant lesions of the cervix. These cervical intraepithelial neoplasia (CIN) are classified from 1-3 in accordance to their severity.
Among the fifteen identified high-risk HPV types, HPV16 and HPV18, are associated with about 70% of cervical cancers. The remaining 30% are caused by other high-risk HPV types.
Both men and women are susceptible for HPV and can develop HPV-associated disorders. Approximately 5% of all cancers worldwide are related to HPV.
Cervical cancer ranks as the 4th most frequent cancer among women in Europe, and the second most common cancer in women 15-44 years of age. It is estimated that each year about 61,000 women from Europe are diagnosed with cervical cancer and about 28,000 women die from the disease. Cervical cancer is preventable in a precancerous state.
The long lag period between the development of precursor lesions and cancer invasion offers the possibility to effectively detect and treat these lesions through cervical cancer screening.
Incidence and mortality are particularly high in Eastern European countries, where the average incidence rate is 16.0 per 100,000 women per year and the mortality rate 6.1 per 100,000 women per year. The variation in cervical cancer incidence can be largely ascribed to differences in cancer screening programs, which vary with respect to interval length, target age groups, quality of screening, level of organization, and coverage.
In countries with a well-organized screening program and high screening participation, cervical cancer incidence rates have shown a substantial decrease in the last decades of the 20th century. Consequently, a disproportionally large number of cancer cases are observed in poorly screened and unscreened women. In contrast, in countries that rely on opportunistic screening and usually have a low screening coverage, cervical cancer incidences have remained high or have even increased.
Developing insights in the cervical pathogenesis and the development of cancer has led to the discovery of several biomarkers, which can be used in different stages of cervical cancer prevention and diagnosis.
Cervical cancer is a public health problem that can be eliminated. In 2018 the World Health Organization called for a global strategy to achieve this: “Through cost-effective, evidence-based interventions, including human papillomavirus vaccination of girls, screening and treatment of precancerous lesions, and improving access to diagnosis and treatment of invasive cancers, we can eliminate cervical cancer as a public health problem and make it a disease of the past.” Dr Tedros Adhanom Ghebreyesus, Director-General, World Health Organization